What commonly causes tingling and numbness?
B12 deficiency — myelin synthesis failure
B12 is a required cofactor for methionine synthase, which converts homocysteine to methionine → SAMe. SAMe is the primary methyl donor for myelin phospholipid synthesis by Schwann cells. When serum B12 drops below ~200 pg/mL, this pathway stalls — myelin repair slows, exposing axons and producing the characteristic stocking-glove tingling pattern. Elevated methylmalonic acid (MMA) confirms functional deficiency even when serum B12 appears borderline
Read more →Peripheral neuropathy — large-fibre vs small-fibre
Large-fibre neuropathy (demyelination) presents as numbness, proprioception loss, and reduced vibration sense — measurable via nerve conduction velocity (NCV) testing. Small-fibre neuropathy (axonal energy failure) presents as burning, pins-and-needles, and temperature hypersensitivity — often normal on NCV but detectable via skin biopsy. The distinction determines whether B12 (myelin repair) or B1 (axonal energy via transketolase) is the priority
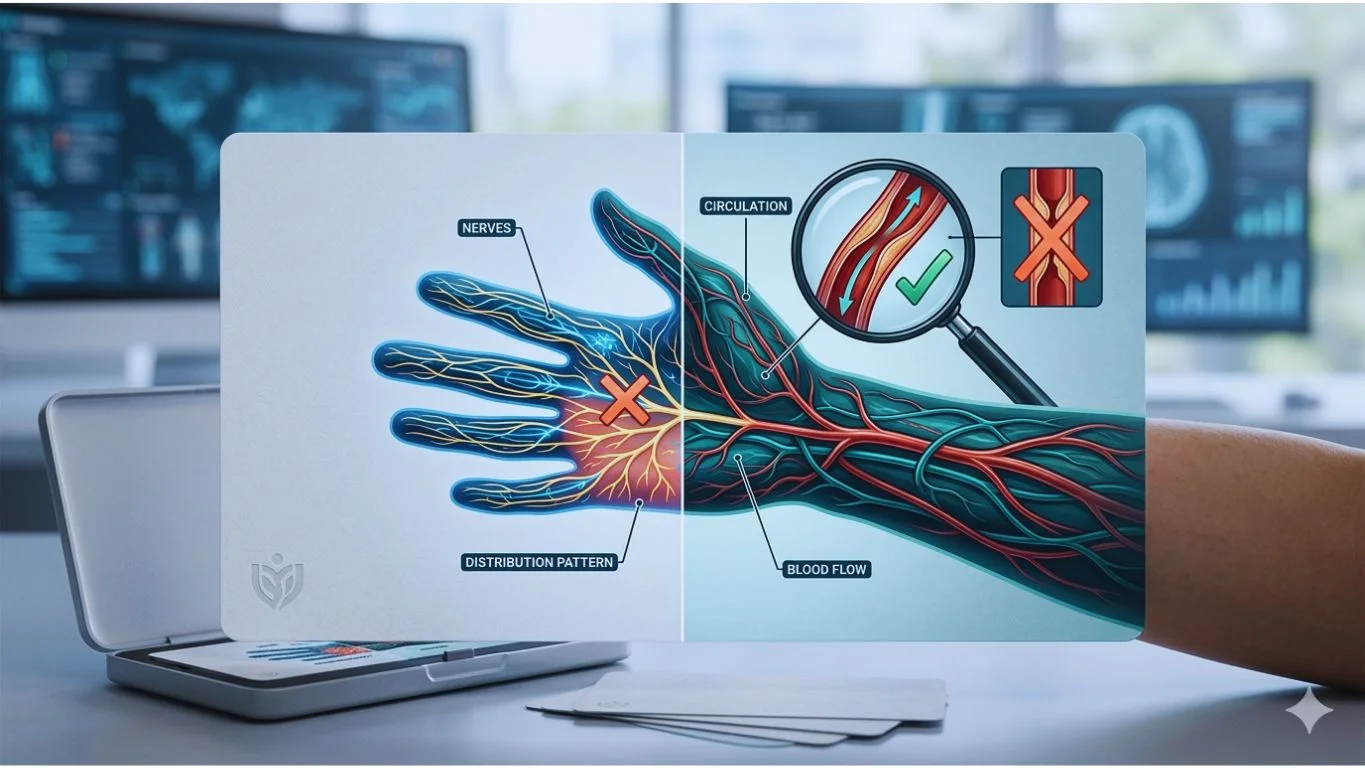
Read more →Neurological vs circulatory tingling — the diagnostic split
Neurological tingling follows nerve dermatome patterns, persists regardless of position, and presents as pins-and-needles or electric sensations. Circulatory tingling is associated with cold extremities, colour changes (pallor → cyanosis → rubor), and resolves rapidly with movement or warming. The distinction matters clinically: nerve tingling points to B12/B1 deficiency or neuropathy; circulatory tingling points to Raynaud's phenomenon or peripheral vascular disease
Read more →When should you see a doctor immediately?
- Sudden numbness on one side of the body
- Tingling accompanied by weakness, vision changes, or slurred speech
- Numbness after a head or neck injury
- Rapidly progressing loss of sensation
These symptoms may indicate a serious condition requiring urgent medical attention
The B12 and tingling connection: SAMe pathway
B12 functions as the essential cofactor for methionine synthase — the enzyme that converts homocysteine to methionine, which is then adenylated to S-adenosylmethionine (SAMe). SAMe is the primary methyl donor for phosphatidylcholine synthesis in Schwann cells, which is the rate-limiting step in myelin membrane assembly. When serum B12 drops below ~200 pg/mL, this pathway stalls: myelin repair slows, existing myelin degrades, and exposed axons generate aberrant electrical signals perceived as tingling
The active form — Methylcobalamin — enters this pathway directly without requiring MMACHC-mediated decyanation (needed for cyanocobalamin) or MTRR-dependent reduction. This bypass is clinically relevant for patients over 50 (reduced gastric intrinsic factor), those on metformin (impaired ileal B12 absorption), or those with MTHFR C677T variants (reduced methyl-cycle efficiency). Early intervention matters: demyelination detected within 6 months is typically reversible; beyond 12 months, axonal loss may become permanent
Understand your symptoms better
How can nerve support supplements help?
The tingling-numbness cycle typically involves two overlapping mechanisms: demyelination (loss of the protective myelin sheath around nerve fibers) and impaired axonal signal conduction. Both processes are B-vitamin-dependent — B12 is a cofactor for myelin synthesis via the methionine synthase → SAMe pathway, while B1 supports energy metabolism within the nerve cell itself
The distinction between active and inactive B-vitamin forms matters here. Standard cyanocobalamin must be converted to methylcobalamin through a multi-step process involving MMACHC and MTRR enzymes. Standard thiamine must be phosphorylated intracellularly. When these conversion pathways are limited — by age, genetics (MTHFR C677T), gut malabsorption, or medication interactions — the nerve tissue receives less usable nutrient despite adequate oral intake
Active forms bypass these bottlenecks: Methylcobalamin enters the methyl cycle directly, Benfotiamine crosses cell membranes via passive diffusion (achieving 5× higher intracellular thiamine levels than standard B1), and P-5-P is the coenzyme form of B6 already active for neurotransmitter synthesis
Clinical context matters. Tingling from acute B12 deficiency often responds within 4–8 weeks of consistent supplementation. Chronic peripheral neuropathy — especially diabetic — may require longer timelines and concurrent medical management. Supplementation supports but does not replace the diagnostic and treatment process
From symptom understanding to targeted support
The symptom patterns on this page — positional tingling, stocking-glove distribution, nocturnal exacerbation — each point to a specific nerve fibre type and mechanism. Large-fibre symptoms (numbness, proprioception loss) correlate with demyelination, where B12-dependent SAMe methylation of myelin phospholipids is the rate-limiting repair step. Small-fibre symptoms (burning, pins-and-needles) correlate with axonal energy failure, where B1-dependent transketolase activity in the pentose phosphate pathway determines Schwann cell ATP production
Cobascore addresses both fibre types simultaneously: methylcobalamin for the myelin repair pathway, benfotiamine for the axonal energy pathway, and P-5-P for neurotransmitter synthesis that modulates pain signal processing. The formula assumes that if you are reading a page about tingling and numbness causes, your situation may warrant more than a general-purpose multivitamin — but confirmation through blood work (serum B12, MMA, homocysteine) remains the clinical standard